





General Information
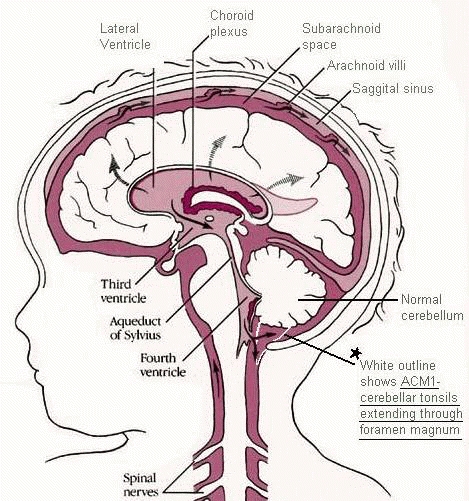
- Chiari malformation is a general term used to describe a condition when the bottom part of the cerebellum (the “tonsils”) dip down into the upper spinal canal.
![]()
![]()
![]()
Causes
- In many cases it is congenital (present at birth). In most cases the compartment of the brain holding the cerebellum (posterior fossa) is smaller than normal.
- If the upper certical vertebra (odontoid process of the second cervical vertebra) ascends into the cranial compartment (basilar invagination), the canal at the junction between the brain and spine can narrow.
- In rare instances high pressure in the brain compartment can “squeeze” the cerebellar tonsils downward. The condition may be associated with the following conditions:
- Pseudotumor cerebri.
- Hydrocephalus (typically due to aqueductal stenosis).
- Brain tumors in the cerebellum.
- Posterior fossa arachnoid cyst.
- In other rare instances, abnormally low pressure in the spinal compartment can “draw” the cerebellar tonsils downward. This can occur in association with the following circumstances:
- Lumboperitoneal shunt.
- Spontaneous intracranial hypotension.
Symptoms
- Pain, especially headache in the back of the head, aggravated by coughing and straining.
- Weakness is also prominent, especially in the hands when there is associated syringomyelia.
- Other symptoms include neck, arm, and leg pain, numbness, loss of temperature sensation, unsteadiness, double vision, slurred speech, trouble swallowing, vomiting and tinnitus (ringing in the ears).
Diagnosis
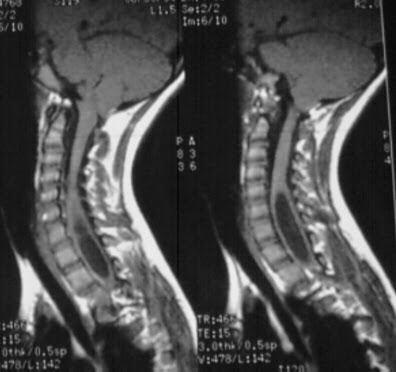
- MRI is the diagnostic test of choice for Chiari I malformation, since it easily shows the tonsillar herniation as well as syringomyelia, which occurs in 20 percent to 30 percent of cases.

- An MRI cerebrospinal fluid (CSF) flow study is often helpful for determining the impact of the Chiari malformation.
- CT-myelogram for diagnosis of spinal CSF leaks for cases of suspected intracranial hypotension, or syringomyelia in the absence of Chiari malformation.
Syringomyelia
Treatment
In general, the surgical aim is to reestablish free flow of cerebrospinal fluid back-and-forth from the brain and spinal compartments. One can think of the cerebellar tonsils as a “cork” that is tightly squeezed into the upper spinal canal “bottle.” Depending upon the anatomy and cause of the Chiari malformation, one or more of the following options can be used:
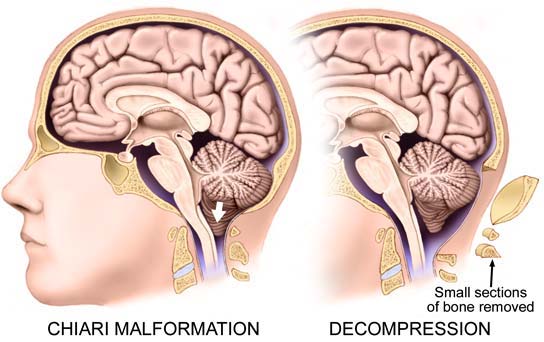
- Posterior fossa decompression.
- The aim is to remove the back, lower part of the skull bone, plus the back of the first cervical vertebra. This widens the “bottleneck” in order to allow CSF flow around the “cork.” This decompression is often accompanied by a duraplasty, a procedure to expose the coverings over the cerebellum, thereby also widening the fluid space.
- Cerebellar tonsillar reduction. Using microsurgical techniques, the lower part of the tonsils can be shrunk down in size so as to reduce the size of the “cork.”
- Removal of the odontoid (part of the second cervical vertebra) in cases in basilar invagination.